Note: This brief was updated on February 27, 2025 to incorporate new data on abortion statistics.
The Supreme Court’s 2022 ruling in Dobbs v. Jackson Women’s Health Organization overturned the constitutional right to abortion that had been in place for nearly 50 years under Roe v. Wade. Prior to the Dobbs ruling, abortions were permitted up to fetal viability in all states. That federal standard was eliminated under Dobbs, allowing states to ban or restrict abortion before viability. KFF is tracking and updating the status of abortion access and availability, with some states banning almost all abortions and some states protecting abortion access.
This issue brief answers some key questions about abortion in the United States and presents data collected before and since the Dobbs ruling.
Abortion is the medical termination of a pregnancy. It is a common medical service that many women obtain at some point in their life. There are different types of abortion methods, which the National Academy of Sciences, Engineering, and Medicine (NASEM) places in four categories:
Decades of research have shown that abortion is a very safe medical service.
Despite its strong safety profile, abortion is the most highly regulated medical service in the country and is now banned in several states. Additionally, many states impose other limitations on abortion that are not medically indicated, including waiting periods and parental notification and consent requirements that typically delay receipt of services.
Since the 2022 Dobbs ruling, abortion has been banned in 13 states, and another 6 states have implemented early gestational limits between 6 and 12 weeks. Most other states allow abortion to the point of fetal viability, which is generally considered around 24 weeks gestation.
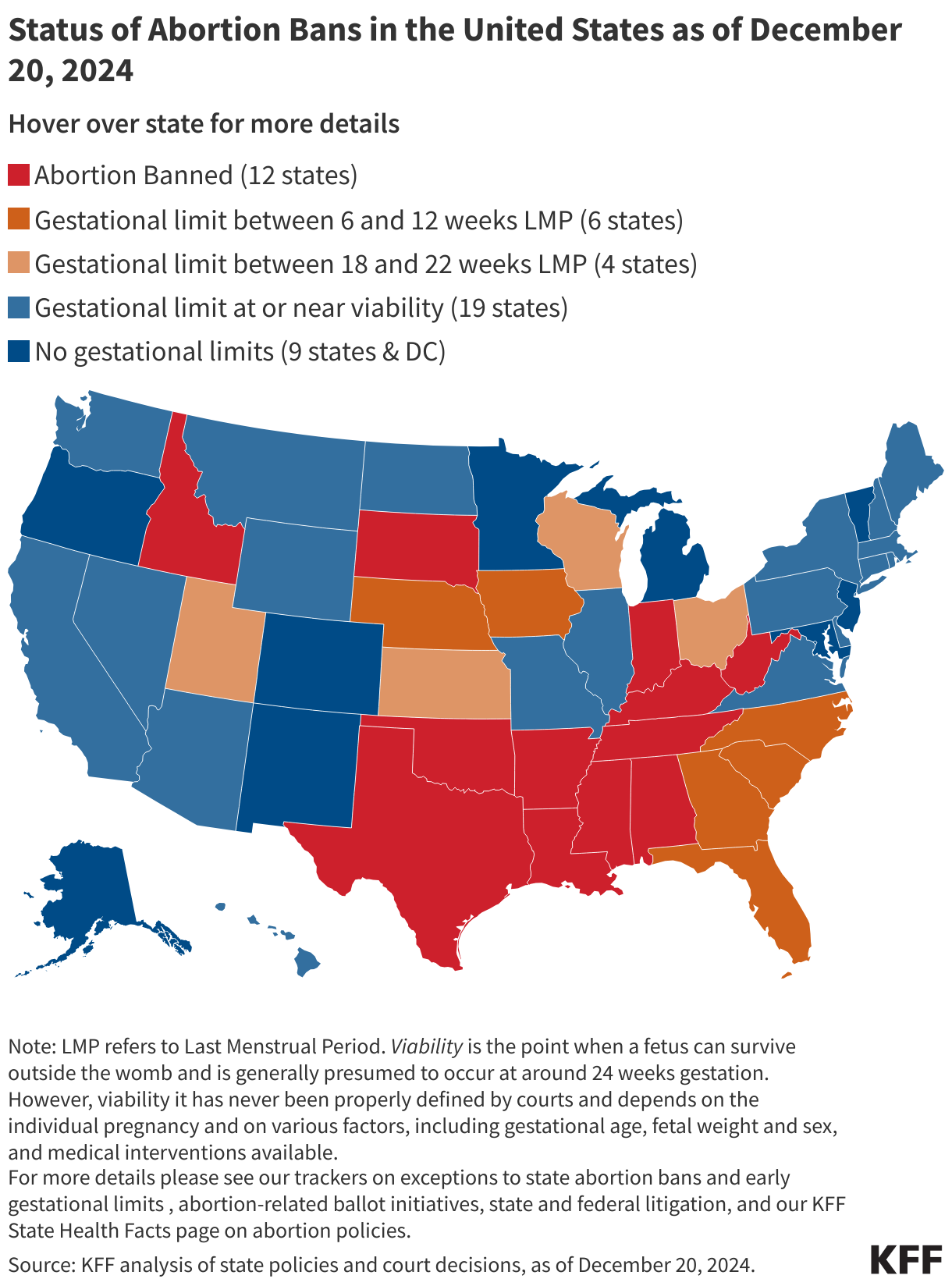
All states that ban abortion have exceptions if an abortion is needed to prevent the death of the pregnant person. Additionally, some state bans make exceptions when the pregnancy is threatening the pregnant person’s health, when the pregnancy is the result of rape or incest, and when there is a lethal fetal anomaly. However, in practice, these exceptions have proven to be unworkable except in the most extreme circumstances. Furthermore, eight states that ban abortion do not make exceptions for cases of rape or incest and six do not have exceptions to protect the health of pregnant people.
(Back to top)
The most recent data estimates that more than one million abortions (1,056,150) occurred in the U.S. in 2023.
Three different organizations currently track abortion volume at the state and the federal levels: the federal Centers for Disease Control and Prevention (CDC), the Guttmacher Institute, and the Society for Family Planning (SFP). The CDC has been collecting abortion data for decades, but several states do not provide data to the federal government (reporting to the CDC is voluntary) and there is a two-to-three-year time lag until the data become publicly available.
Since the Dobbs ruling, the Guttmacher Institute’s Monthly Abortion Provision Study and the SFP’s #WeCount have been tracking state level changes in abortion volume based on data provided by abortion clinics and providers. Both studies provide national and state-level estimates on procedural and medication abortions but differ in some methodologic details. The Guttmacher study compares current abortion rates to 2020, while #WeCount compares rates to the months immediately before Dobbs in 2022. Neither source includes data on self-managed abortions, which are abortions that a pregnant person can do on their own by taking medication abortion pills without clinical supervision. For more details about data sources, see KFF’s issue brief on abortion trends.
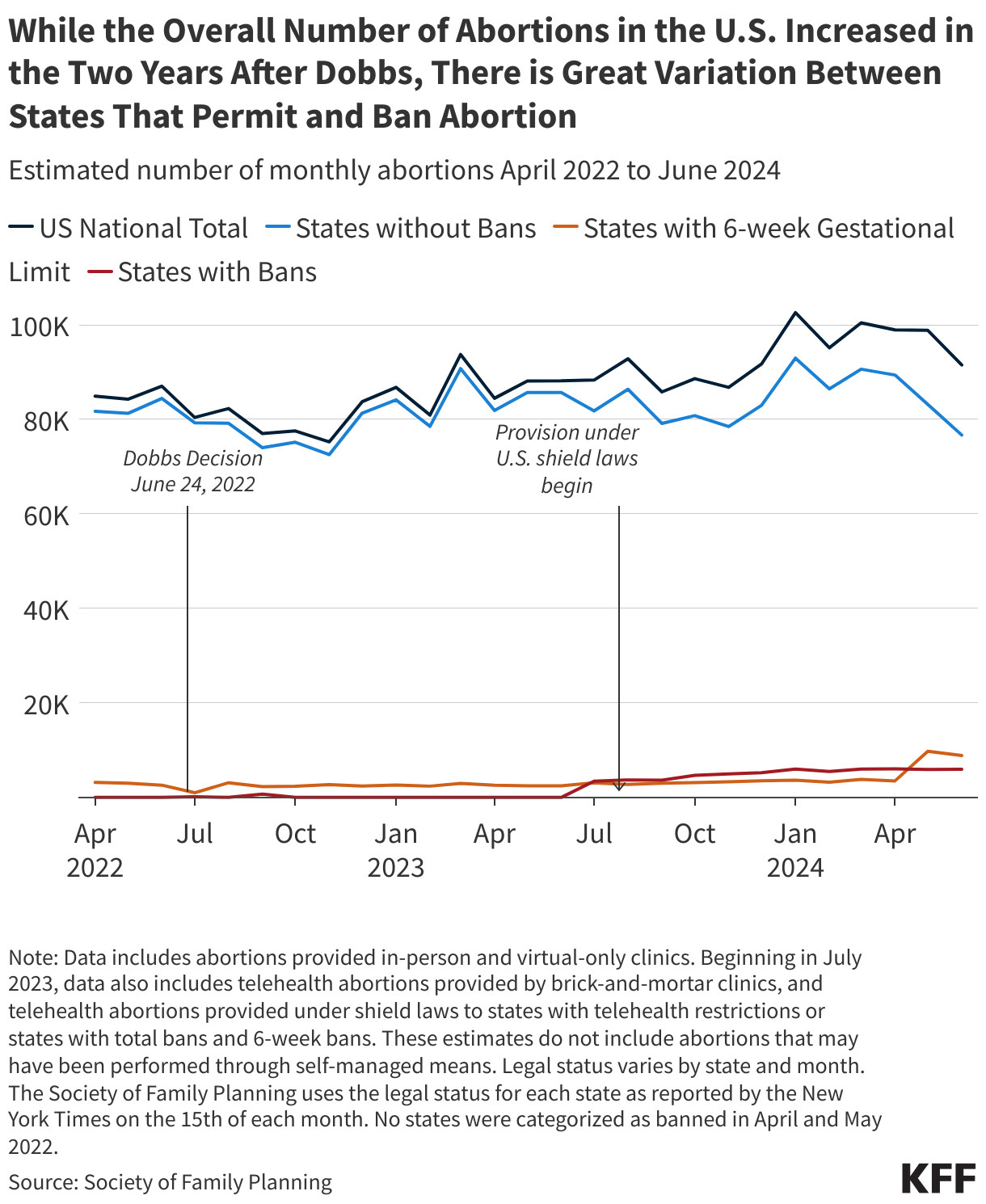
For most of the decade prior to the Dobbs ruling, there was a steady decline in abortion rates nationally, but there was a slight increase in the years just before the ruling. Immediately following the Dobbs ruling, the number of abortions in the U.S. dropped as more states enforced bans and restrictions.
Paradoxically, the most recent data show that the abortion volume in the U.S. slightly increased overall in the two years following the Dobbs ruling. However, the small upswing nationally obscures the massive declines in abortion care provided in states with bans.
In the first six months of 2024, the national abortion volume averaged 98,000 abortions per month, higher than the monthly averages before the Dobbs decision. There are month-to-month variations in all states, and changes in policy can cause larger shifts. For example, in May 2024 Florida implemented a ban on abortions after six weeks gestation (previously permitted up to 15 weeks), and subsequently there was a noticeable decline in abortions in the state and nationally.
States without abortion bans experienced an increase of abortions in the two and a half years since the Dobbs ruling likely due to a combination of reasons: increased interstate travel for abortion access, expanded in-person and virtual/telehealth capacity to see patients, increased measures to protect and cover abortion care for residents and out-of-state patients, and the broader availability of low-cost abortion medication. However, the aggregate increase nationally masks the sharp decline in abortions provided in states with total bans or severe restrictions as well as the hardships that many pregnant people experience in accessing abortion care. In states with bans, abortions are near zero.
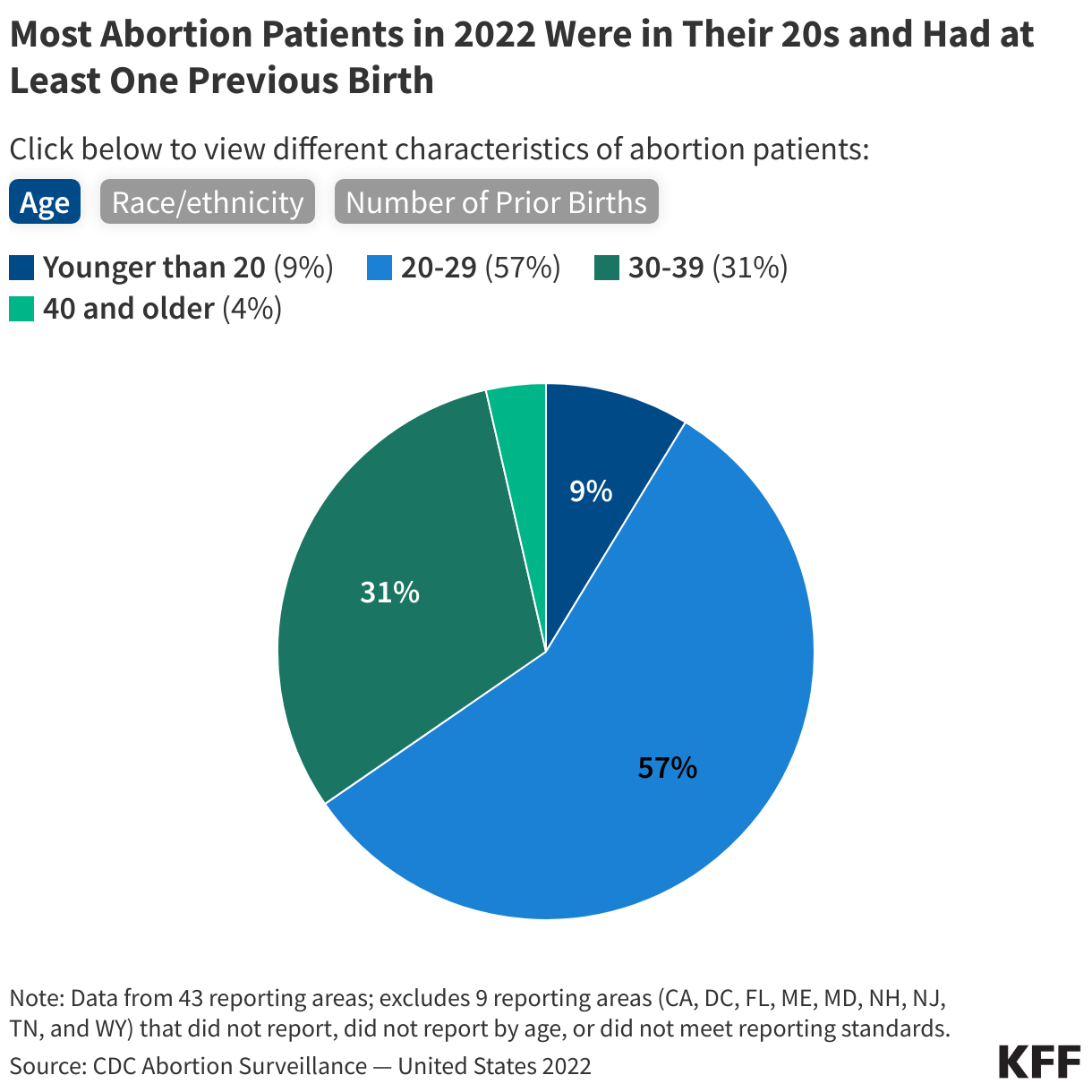
Most of the information about people who receive abortions comes from CDC data. In 2022, women across a range of age groups, socioeconomic status, and racial and ethnic backgrounds obtained abortions, but the majority were obtained by women who were in their twenties, low-income, and women of color.
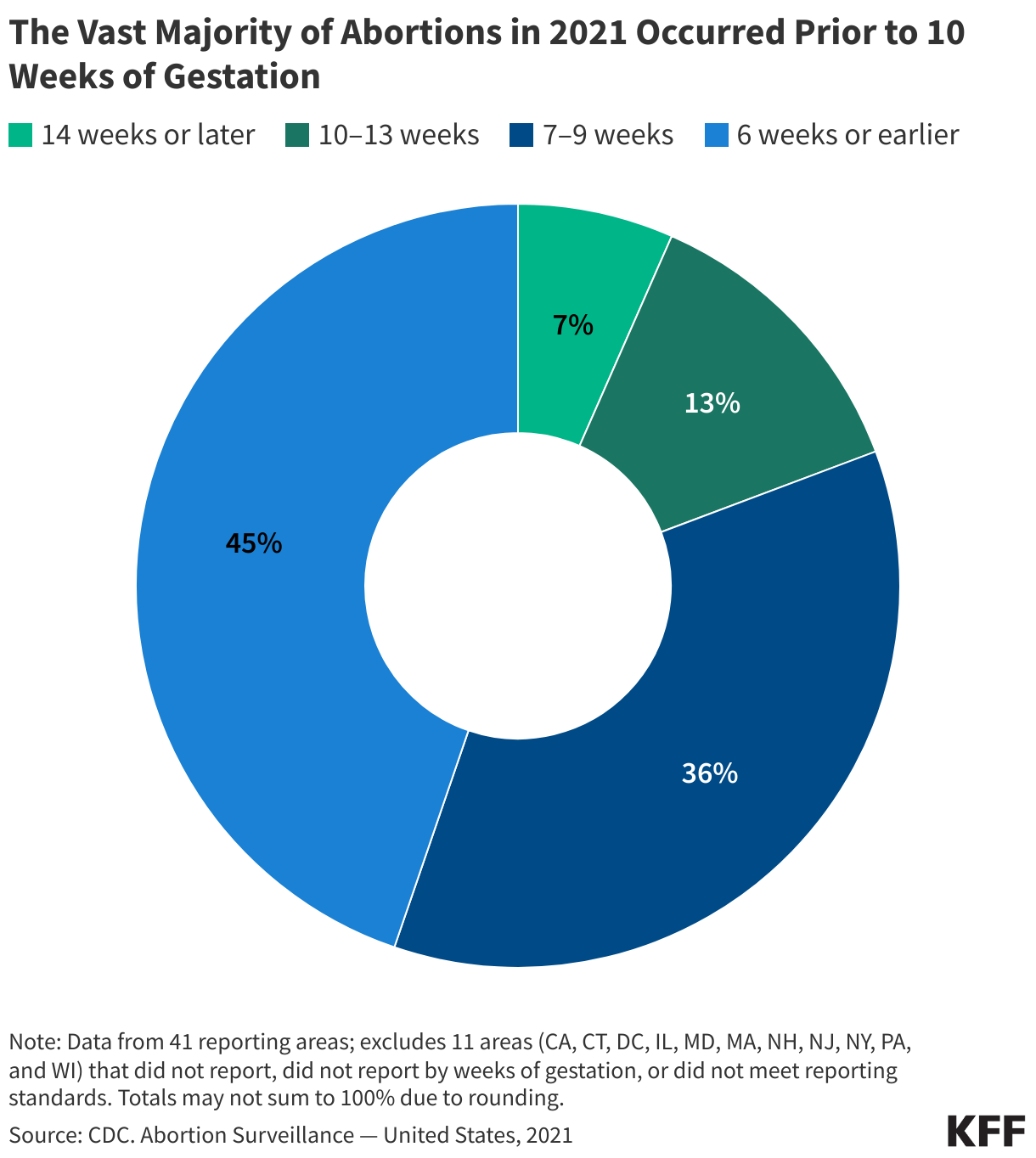
The vast majority (93%) of abortions occur during the first trimester of pregnancy according to data available from before the Dobbs decision.
Before the 2022 ruling in Dobbs, there was a federal constitutional right to abortion before the pregnancy is considered to be viable, that is, can survive outside of a pregnant person’s uterus. Viability is generally considered around 24 weeks of pregnancy. Most abortions, though, occur well before the point of fetal viability. When people have abortions later in pregnancy, it is often because the fetus is not viable and the pregnancy may endanger the pregnant person’s life.
Just over half of abortions were provided at clinics that specialize in abortion care in 2020. Others were provided at clinics that offer abortion care in addition to other family planning services.
The Guttmacher Institute estimates that 96% of abortions were provided at clinics and just 4% were provided in doctors’ offices or hospitals in 2020. Most clinic-based abortions were provided at clinics that specialize in providing abortion care, but many were provided at clinics that offer a wide range of other sexual and reproductive health services like contraception and STI care. Most abortions are provided by physicians. However, in 19 states and D.C., Advanced Practice Clinicians (APCs) such as Nurse Practitioners and midwives may provide medication abortions. Conversely, 31 states prohibit clinicians other than physicians from providing abortion care.
Many clinics stopped offering abortion services shortly after the Dobbs ruling, but contrary to expectations, the number of abortions conducted by abortion-providing facilities increased overall since the ruling. However, the distribution of these facilities varies widely by state and geographic region, and the increase is largely driven by the expansion of virtual abortion clinics. While virtual clinics can remove geographic barriers for those seeking abortion care, their services are limited to medication abortion. Brick-and-mortar clinics can offer medication abortion, procedural abortions, and services for abortions later in pregnancy. However, the overall number of brick-and-mortar independent clinics has decreased over the years, with over 75 independent abortion clinics shutting down between 2022 and 2024.
Even prior to the ruling in Dobbs, access to abortion services was very uneven across the country. The proliferation of restrictions in many states, particularly in the South, had greatly shrunk the availability of services in some areas. In the wake of overturning Roe v. Wade, these geographic disparities have only widened.
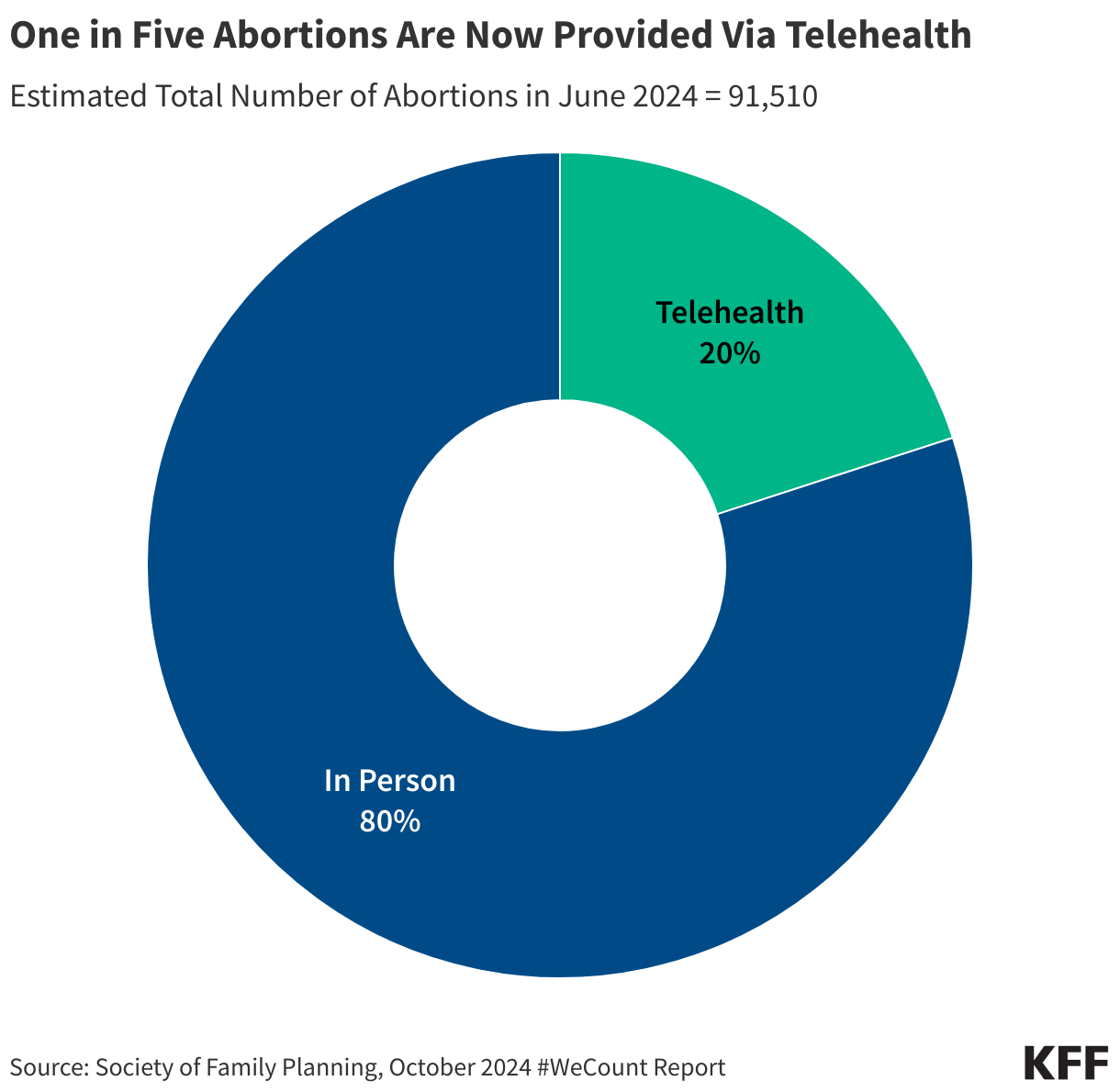
Telehealth has grown as a delivery mechanism for abortion services. While procedural abortions must be provided in person in a clinical setting, medication abortion can be provided in a clinical setting or via telehealth without an in person visit. Access to medication abortion via telehealth had been limited for many years by an FDA restriction that permitted only certified clinicians to dispense mifepristone within a health care setting. In December 2021, however, the FDA permanently revised this policy and no longer requires clinicians to dispense the drug in person. Additionally, in January 2023, the FDA finalized a policy change that allows retail pharmacies to dispense medication abortion pills to patients with a prescription. These policy changes opened the door to using telehealth for medication abortion.
Self-managed abortions typically involve obtaining medication abortion pills from an online pharmacy that will send the pills by mail or by purchasing the pills from a pharmacy in another country, usually without the involvement of a physician or advanced practice clinician. While this can involve asynchronous contact with non-US-based clinicians, it does not typically involve a direct consultation with a clinician either in person or via telehealth.
It is difficult to track the volume of self-managed abortions since they are outside of the formal health care system, and it is unknown if all people who receive medication pills take them. One study estimated that at least 26,000 additional self-managed medication abortions took place in the six months following the Dobbs ruling. More than half of self-managed medication abortions pills were distributed through volunteers in community networks, while others were provided by telehealth organizations outside the formal U.S. health care system and online vendors.
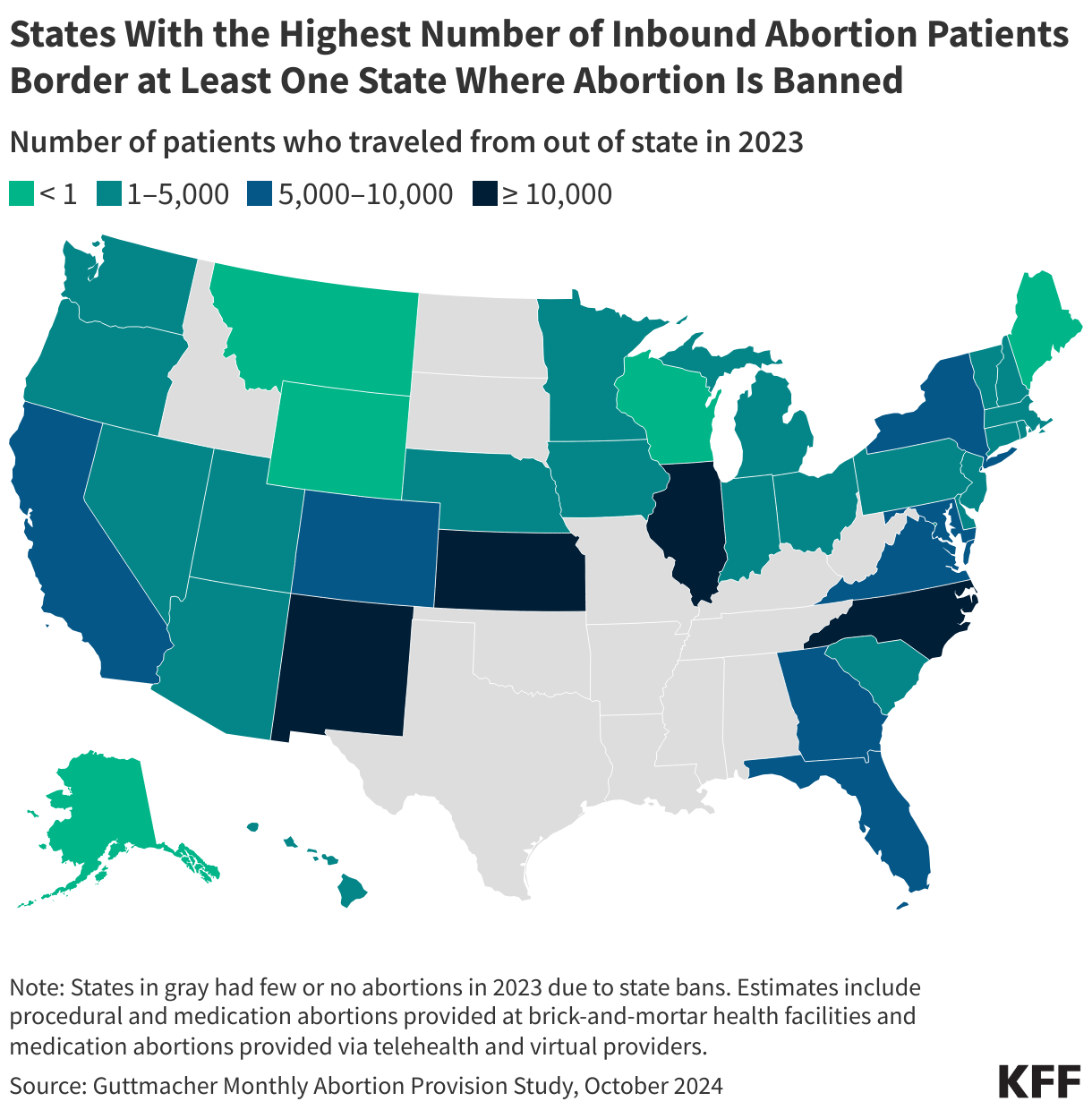
The Guttmacher Institute Monthly Abortion Provision Study is the only data source so far to provide in-depth information on interstate travel pre- and post-Dobbs. Guttmacher estimates that prior to Dobbs, nearly one in ten people obtained an abortion by traveling across state lines in 2020. Even before Roe v Wade was overturned, abortion was highly restricted in many states. The latest data from 2023 show that the interstate travel rate for abortion care more than doubled in 2023, with approximately one in five (~171,000) abortion patients traveling out of state for care in 2023 compared to 74,000 in 2020.
Illinois experienced the largest increase in inbound travel for abortion care, with an estimated 37,000 abortion patients traveling into the state in 2023. North Carolina, New Mexico, and Kansas also experienced a rise in the number of out-of-state abortion patients during this time.
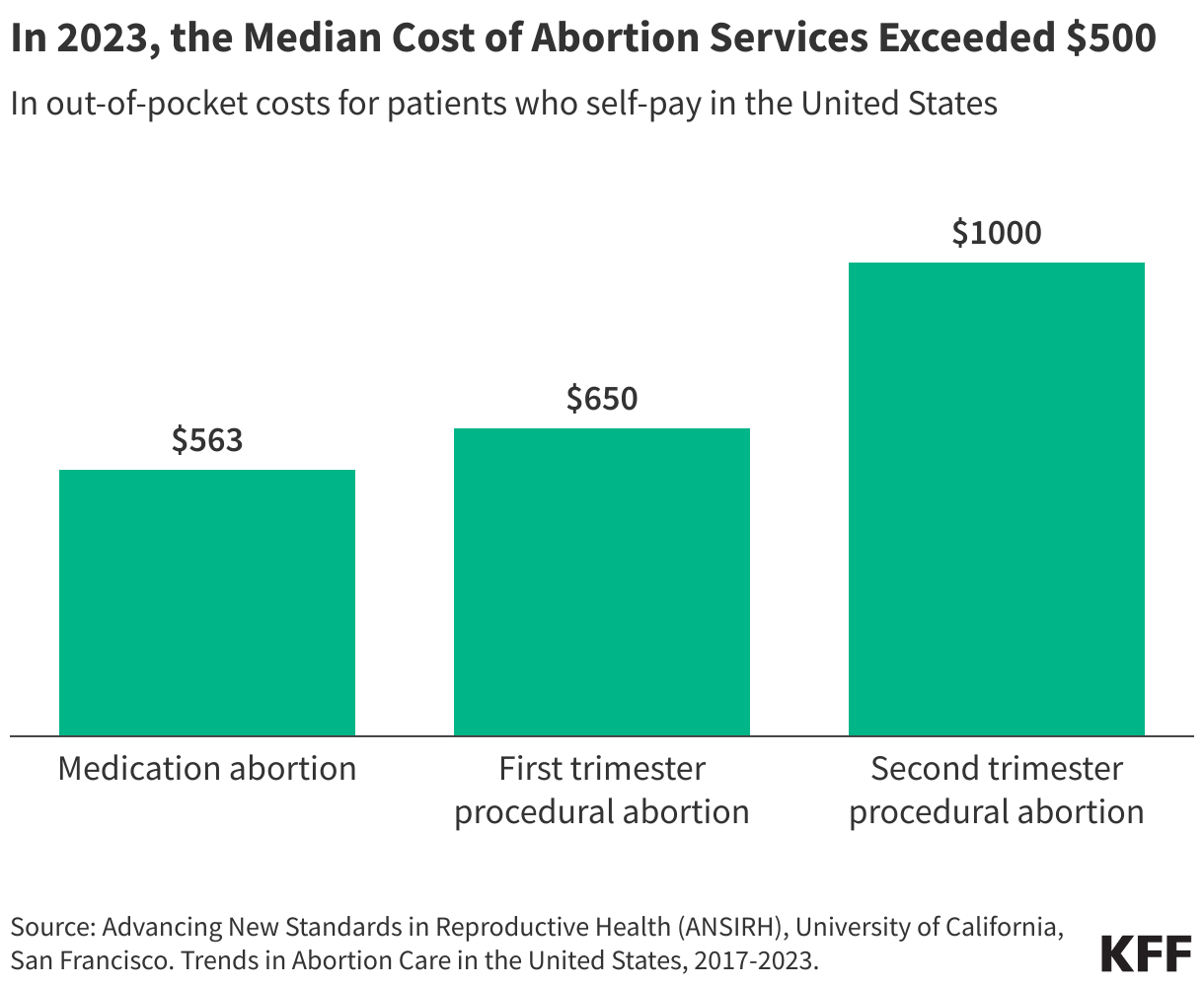
The costs of abortion services vary depending on the method and can exceed $500.
Insurance coverage for abortion services is heavily restricted in certain private insurance plans and public programs like Medicaid and Medicare.
Among women of reproductive age, approximately one in three are covered by private insurance, one in five are covered by Medicaid, and one in ten are uninsured. States regulate fully-insured private plans in their state, whereas the federal government regulates self-funded plans. States can choose whether abortion coverage is included or excluded in private plans that are not self-funded.
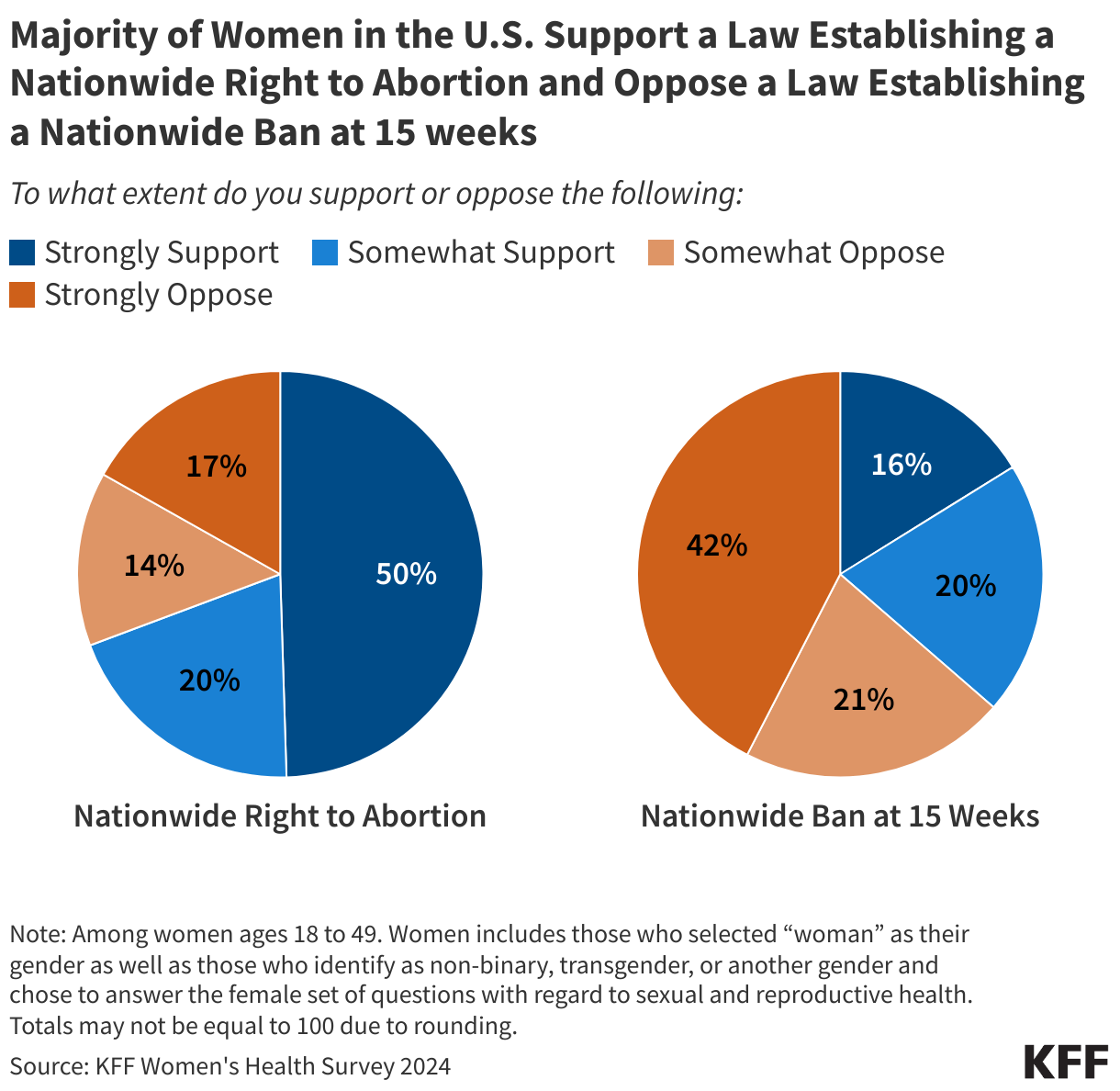
KFF’s national polls have consistently found that a majority of the public did not want to see Roe v. Wade overturned and that most people feel that abortion is a personal medical decision. Similarly, findings from the 2024 KFF Women’s Health Survey show 70% of women of reproductive age—the age group that is most directly impacted by state abortion policies—support a nationwide right to abortion.
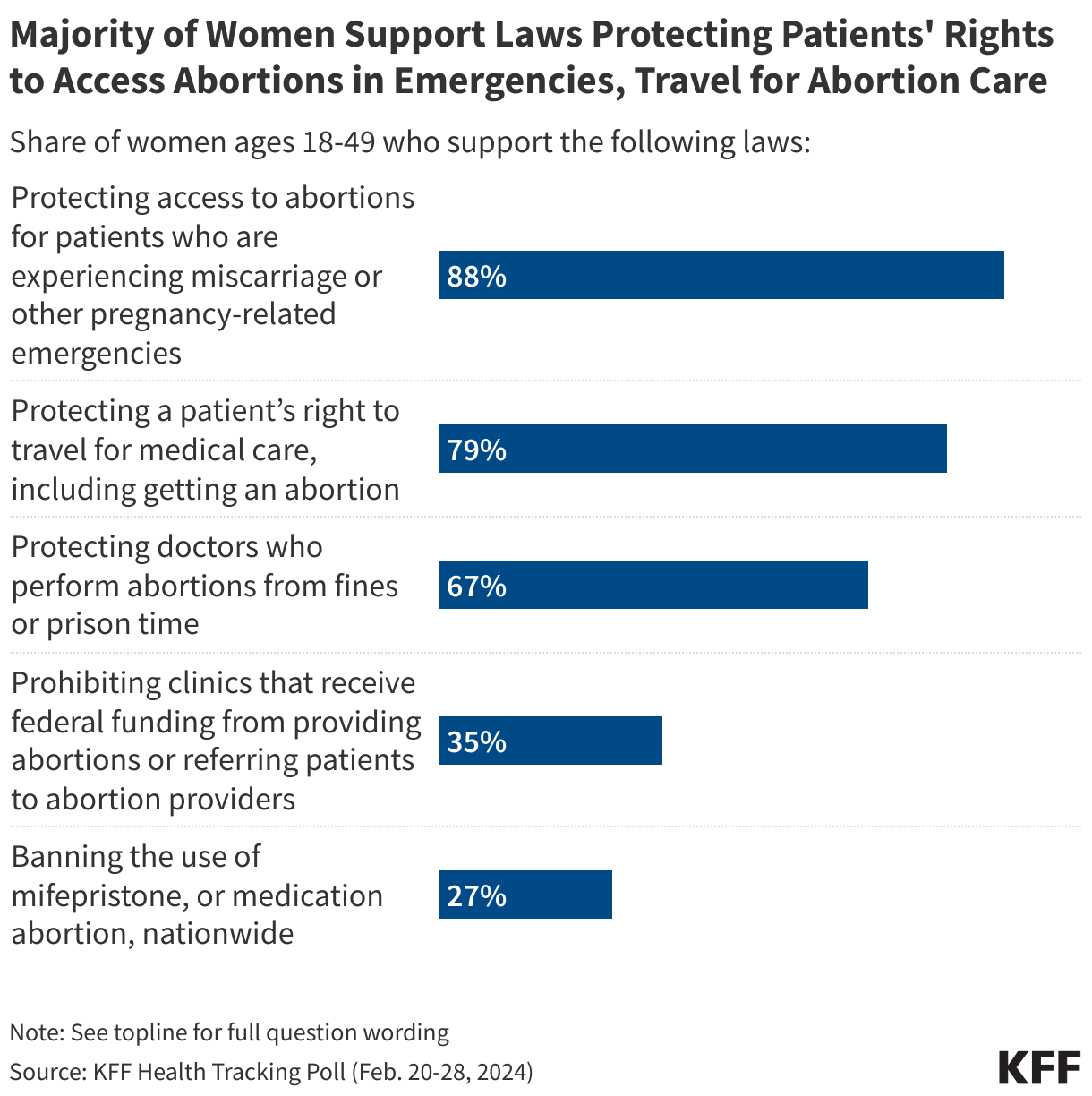
Furthermore, much of the public supports access to abortions for patients who are experiencing pregnancy-related emergencies (88%), a patient’s right to travel for abortion care (79%), and protecting doctors who perform abortions from legal penalties (67%).




Leave a comment